How Effective Are Georgia Lawyer Program Substance Abuse?
Georgia attorneys struggling with alcohol or drug problems have access to a real, structured support system through the State Bar’s confidential programs.
The Georgia Lawyer Assistance Program offers 24/7 counselor access, six prepaid clinical sessions per year, and peer support through Georgia Lawyers Helping Lawyers, all designed to lower the barriers that keep lawyers from asking for help.
This article breaks down how those programs work, what the evidence says about their effectiveness, and what attorneys should realistically expect.
Confidential Programs for Attorneys with Substance Use Disorders in Georgia
Lawyers face behavioral health challenges at rates that exceed many other professions. About 21% of licensed attorneys in a 2016 national study involving 19 states, including Georgia, qualified as problem drinkers. Younger lawyers in their first decade of practice showed even higher rates. Depression, anxiety, and chronic stress compound the picture.
Yet attorneys are often the last professionals to seek help. The reasons are specific to legal culture: fear of losing clients, fear of peer stigma, fear of discipline, and fear that disclosed impairment will be read as professional unreliability. Georgia’s confidential attorney support system is built around those fears.
Understanding what it actually offers, and where it falls short, matters for any lawyer weighing whether to reach out.
How the Georgia Lawyer Assistance Program Works?
The State Bar of Georgia’s Lawyer Assistance Program is a confidential service for Bar members, administered through SupportLinc and managed by CuraLinc Healthcare. It is not a lawyer referral service and is not open to the general public.
Members get six prepaid clinical sessions per calendar year at no cost, delivered by an independent, fully licensed counselor near their office or home.
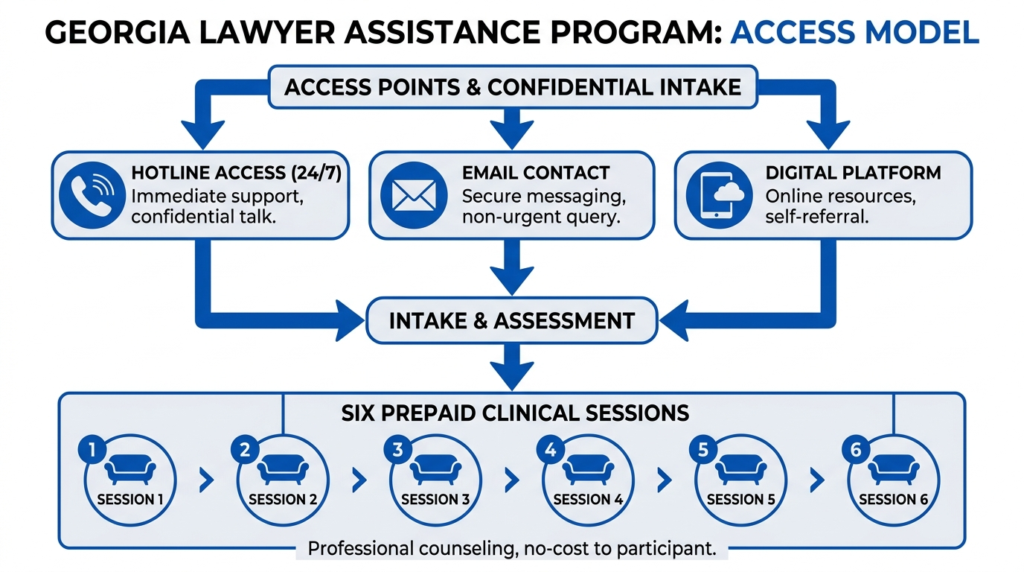
Access is available through multiple channels:
- A 24/7 hotline staffed by trained counselors at 800-327-9631
- Email at gabar@curalinc.com
- A digital portal with scheduling, assessments, and online support tools
The digital platform also includes text therapy, virtual group support, and digital cognitive behavioral therapy that can target substance use, stress, depression, anxiety, and sleep problems. That range of entry points is deliberate. Lawyers with emerging alcohol or drug problems often do not identify first as “impaired.”
They may recognize burnout, insomnia, or family strain before they name the underlying issue. Georgia’s broad framing, which places substance abuse alongside stress, depression, and workplace conflict, creates softer entry points into care.
Why Third-Party Administration Matters?
Georgia routes initial counseling contact through an outside clinical vendor rather than directly through Bar staff.
The Korean-American Bar Association of Georgia notes that LAP is provided through a third-party counseling agency specifically to protect confidentiality. Callers are asked for information but are not required to provide it, and anything they share is kept strictly confidential.
That structural separation is not just administrative. For a lawyer afraid that seeking help might somehow reach the Office of the General Counsel, knowing that the first clinical contact is with an outside healthcare company, not a Bar employee, can make the difference between calling and not calling.
What Confidentiality Actually Means in Georgia?
Georgia’s confidentiality protections for attorneys seeking treatment are layered and genuinely strong, but they are not absolute.
The Georgia Department of Behavioral Health and Developmental Disabilities publishes a formal HIPAA-based Notice of Privacy Practices governing how protected health information may be used or disclosed. Attorneys receiving care through DBHDD-governed providers are protected within that framework.
Georgia also has unusually strong mental health privilege protections. Analysis of O.C.G.A. § 24-5-501 and related case law describes psychiatrist-patient privilege in Georgia as “almost an absolute privilege,” subject only to narrow exceptions or waiver. Substantive communications with covered mental health providers are heavily protected, though the fact that treatment occurred and the dates of treatment may carry less protection in some contexts.
Substance use treatment records often carry additional federal protection under 42 C.F.R. Part 2 for federally assisted programs. In 2026, the Office for Civil Rights launched a civil enforcement program for Part 2 confidentiality, aligned with HIPAA enforcement mechanisms including complaints, investigations, corrective action plans, and civil penalties.
For Georgia attorneys whose treatment providers fall under Part 2, confidentiality is now backed by more explicit federal enforcement than it was even a few years ago.
That said, confidentiality is not the same as immunity. Georgia’s disciplinary system can confidentially refer a lawyer for a medical or mental health evaluation under Bar Rule 4-104 if signs of substance abuse appear during an investigation.
If a lawyer poses a substantial threat of harm to clients or the public, Bar Rule 4-108 allows the State Disciplinary Board to seek emergency suspension. Once probable cause leads to a formal hearing before a special master, proceedings become public in the Supreme Court of Georgia.
The practical line is this: LAP is confidential at the entry stage, but untreated impairment that produces client harm, dishonesty, or noncooperation can trigger a separate regulatory process that moves toward public accountability.
The Treatment Infrastructure Behind Attorney Referrals
Georgia’s attorney support programs are not a standalone clinic. When a lawyer’s needs exceed six short-term counseling sessions, the likely next step is referral into Georgia’s broader licensed treatment network.
Effective January 1, 2026, House Bill 584 transferred licensing and oversight of several key facility types, including Drug Abuse Treatment and Education Programs, Narcotic Treatment Programs, and Adult Residential Mental Health Programs, from the Department of Community Health to DBHDD. That consolidation means treatment provider oversight is now more unified under the specialized behavioral health agency.
Georgia’s Narcotic Treatment Program rules require compliance with SAMHSA, DEA, and Georgia Board of Pharmacy standards, licensed and qualified medical staff, and certified counselors. NTPs must also report serious patient incidents to the Department within 24 hours.
The general licensing and enforcement rules governing these facilities define investigations broadly and include review of premises, staff, and documents relevant to licensing.
For attorneys, this matters because the quality of rehabilitation depends not only on Bar intake but on the regulatory accountability of the providers to whom lawyers are referred.
Georgia Lawyers Helping Lawyers: The Peer Support Layer
Alongside the clinical program, Georgia runs a separate confidential peer-to-peer program called Georgia Lawyers Helping Lawyers. The Supreme Court of Georgia approved amendments to the State Bar’s rules in November 2025 that formalized this program’s standing within the Bar’s structure.
Peer support serves a different function from counseling. It reduces stigma, creates profession-specific trust, and can engage lawyers who are not yet ready for formal treatment. Some attorneys will tell another lawyer the truth before they tell a therapist, a managing partner, or a spouse. Georgia’s two-lane model recognizes that reality.
| Component | Primary function | Why it matters for substance use |
|---|---|---|
| LAP clinical sessions | Triage, short-term counseling, referral | Removes cost barrier and provides immediate professional help |
| 24/7 hotline | Crisis and after-hours access | Supports help-seeking at the moments it actually happens |
| Digital platform | Scheduling, CBT, virtual groups | Allows discreet, low-visibility engagement |
| Lawyers Helping Lawyers | Confidential peer-to-peer support | Overcomes profession-specific shame and stigma |
How Effective Are These Programs? What the Evidence Shows
This is the central question, and the honest answer is that Georgia’s programs are credible and well-designed at the access stage, but their effectiveness for severe substance use disorders is not publicly documented.
Georgia does not publish annual LAP outcome data. There are no public figures for the number of attorney participants, referrals to residential or intensive outpatient treatment, completion rates, relapse rates, or return-to-practice outcomes. That absence is itself a meaningful finding.
California offers a useful comparison. The California LAP 2018 annual report showed 148 new participants, 276 total participants, and 144 closed cases, with 41% of cases closed after participants met stated program goals and only one case terminated for noncompliance.
The 2022 California report showed similar results, with 42% of 165 closed cases meeting stated goals. California also reported that 49% of participants presented with substance use disorder, 23% with mental health concerns only, and 24% with both.
Florida takes a different approach, emphasizing structured monitoring. The Florida Lawyers Assistance program monitors law students, conditionally admitted attorneys, and lawyers on diversion or probation, using random drug testing, weekly attorney support meetings, monthly mentor reports, and facilitated groups. Florida also explicitly links chemical dependency treatment to disciplinary mitigation after Supreme Court decisions recognized recovery as a mitigating factor.
National evidence supports the broader value of these programs. A 2001 Oregon study cited by the National Conference of Bar Examiners found that malpractice and discipline complaint rates for impaired lawyers were nearly four times as high before treatment as after treatment.
That is indirect evidence for Georgia, but it supports the proposition that rehabilitation and monitoring can meaningfully reduce professional harm.
Georgia compares well on confidential access and front-end usability. It compares less favorably on publicly documented long-term recovery management and outcome transparency. California is strongest in public accountability.
Florida is strongest in integration of monitoring with discipline and admissions systems. Georgia appears strongest in privacy-focused, low-barrier entry.
Why the Lack of Outcome Data is Not a Neutral Issue?
A confidential program can be well-designed and clinically useful while still being impossible to evaluate externally. Georgia’s official materials explain access clearly but do not show what happens when a lawyer needs more than six sessions, more than peer support, and more than a digital behavioral health platform.
That gap matters most for the attorneys at highest risk. A lawyer with emerging stress-related drinking may do well with six sessions and peer contact.
A lawyer with alcohol dependence, opioid misuse, or a pattern of relapse needs a clear pathway to higher levels of care, documented treatment linkages, and some form of ongoing accountability. Georgia’s public materials do not describe that pathway in detail.
The California Lawyer Assistance Program explicitly serves State Bar applicants and offers monitored services as needed. Florida explicitly monitors conditionally admitted attorneys and those on diversion. Georgia’s publicly visible materials do not show this level of admissions-linked or discipline-linked rehabilitation architecture.
This is not a condemnation of Georgia’s program. It is a call for transparency proportionate to the seriousness of lawyer impairment and public protection.
What Georgia Attorneys Should Know in Practice?
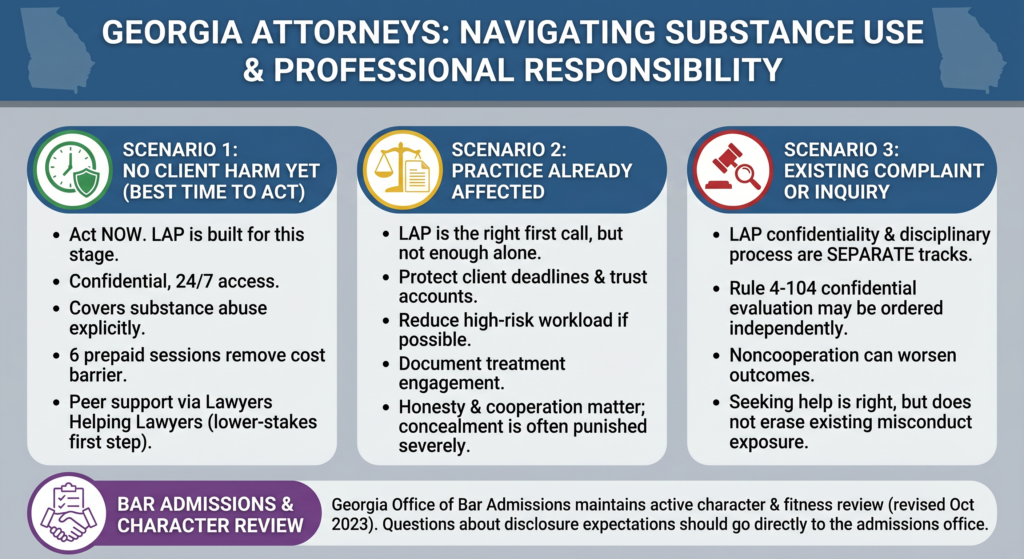
If you are a Georgia lawyer worried about your drinking or drug use and no client harm has occurred yet, the best time to act is now. Georgia’s LAP is built for exactly this stage.
The program is confidential, available around the clock, and covers substance abuse explicitly. Six prepaid sessions remove the initial cost barrier, and peer support through Lawyers Helping Lawyers offers a lower-stakes first conversation if shame is the main obstacle.
If your substance use is already affecting your practice, LAP is still the right first call, but it is not enough on its own. Protect client deadlines and trust-account functions. Reduce high-risk workload if you can. Document your treatment engagement. The profession often punishes concealment more severely than the original performance decline, so honesty and cooperation matter.
If there is already a client complaint or disciplinary inquiry, understand that LAP’s confidentiality and the disciplinary process are separate tracks. A confidential evaluation under Rule 4-104 may be ordered independently. Noncooperation can worsen outcomes. Seeking help is still the right move, but it does not erase existing misconduct exposure.
For applicants with mental health or substance use histories, the Georgia Office of Bar Admissions maintains an active character and fitness review process, revised in October 2023. Questions about disclosure expectations should go directly to the admissions office.
Georgia’s System is Real, But Needs More Transparency
Georgia’s confidential attorney rehab framework is credible, accessible, and privacy-conscious at the intake stage.
The State Bar has made thoughtful design choices: outsourced administration, 24/7 access, peer support, digital tools, and broad wellbeing framing that normalizes help-seeking before crisis. The treatment providers attorneys are referred to operate within a regulated, inspected system now consolidated under DBHDD.
What Georgia has not yet done is show the public whether those design choices translate into recovery. Annual outcome reporting, clearer referral pathways for severe addiction, and a plain-language explanation of how voluntary treatment interacts with discipline and admissions would all strengthen the system’s credibility with the attorneys most afraid to use it.
The most accurate bottom line is this: Georgia’s programs are well-designed for early intervention and first contact, but only modestly proven as a long-term rehabilitation system because the Bar does not publish enough outcome data to demonstrate effectiveness at scale.
For attorneys, that means using the system early, treating it as a first step rather than a complete solution, and being prepared to seek more intensive care if the problem is serious.
If you are a Georgia attorney and ready to take that first step toward confidential, professional support, Thoroughbred’s attorney addiction programs offer a full continuum of care, from medical detox through outpatient treatment, designed for working professionals who need real help without sacrificing their careers.