2-MMC: Effects, Side Effects, and Overdose Risks
2-MMC is a synthetic cathinone stimulant that has rapidly emerged in European drug markets as a replacement for controlled substances like 3-MMC and mephedrone.
About half of powders sold as 3-MMC in early 2024 actually contained 2-MMC, meaning many users consume this drug without knowing it.
This article explains what 2-MMC does to your body, the serious side effects you need to watch for, and why overdose risk is higher than many people realize.
What is 2-MMC and Why It Matters?
2-Methylmethcathinone, known as 2-MMC, is a laboratory-made stimulant chemically related to cathinone, the psychoactive compound found naturally in khat plants. The European Union Drugs Agency brought 2-MMC under EU-wide legal control in January 2026 after monitoring showed it was replacing previously banned cathinones in the illicit market.
This substance belongs to the methylmethcathinone family alongside 3-MMC and 4-MMC (mephedrone). These compounds share similar chemical structures but differ in how they affect brain chemistry and how long their effects last. The position of a single methyl group changes the drug’s potency, duration, and risk profile.
What makes 2-MMC especially concerning is not just its pharmacology but how it reaches users. Drug-checking services across 10 EU countries found that around half of products sold as 3-MMC in the first half of 2024 actually contained 2-MMC instead. This widespread mislabeling means people often take 2-MMC when they think they are using something else, making dose estimation unreliable and overdose more likely.
How 2-MMC Works in the Brain?
A 2025 systematic review concluded that 2-MMC and 3-MMC have pharmacological profiles broadly similar to mephedrone, with comparable dopaminergic activity but less serotonergic action. This means 2-MMC primarily increases dopamine and norepinephrine in the brain, producing stimulant effects like increased energy, alertness, and euphoria.
The drug works by interacting with monoamine transporters, the proteins responsible for clearing neurotransmitters from the space between brain cells. When 2-MMC blocks or reverses these transporters, dopamine, norepinephrine, and to a lesser extent serotonin accumulate in the synapse, amplifying their effects on mood, arousal, and reward circuits.
Research on mephedrone shows it functions as a nonselective monoamine releaser with relatively greater dopamine transporter affinity than MDMA. Because 2-MMC appears pharmacologically similar but with even less serotonergic activity, it likely produces a more purely stimulant experience with less of the empathogenic or prosocial effects associated with MDMA.
Short Duration Drives Repeated Use
One of the most important characteristics of 2-MMC is its short duration of action. The systematic review specifically notes that 2-MMC and 3-MMC have shorter durations than mephedrone, which increases craving and encourages frequent redosing within a single session.
This pattern creates a dangerous cycle. When desired effects fade quickly, users feel compelled to take another dose to maintain the high.
Each redose adds to the total drug load in the body, increasing cardiovascular strain, hyperthermia risk, and the likelihood of severe toxicity. The short action also makes 2-MMC particularly habit-forming because the rapid reward-decline-reward cycle strengthens compulsive use patterns.
Effects of 2-MMC: What Users Experience?
Based on evidence from closely related cathinones and the limited direct data available, 2-MMC likely produces effects similar to other methylmethcathinones but with a stimulant-heavy profile.
Desired Effects
People use 2-MMC seeking stimulant and sometimes entactogenic effects that overlap with MDMA, cocaine, and amphetamine. Common desired effects include:
- Increased energy and wakefulness
- Euphoria and elevated mood
- Enhanced sociability and confidence
- Reduced fatigue
- Increased motivation to move, dance, or socialize
- Possible disinhibition and increased libido in some contexts
These effects are driven primarily by increased dopamine and norepinephrine activity, which activate reward circuits and arousal systems in the brain.
Physical Effects
On the body, 2-MMC produces typical sympathomimetic stimulant effects:
- Increased heart rate (tachycardia)
- Elevated blood pressure (hypertension)
- Dilated pupils
- Sweating and increased body temperature
- Dry mouth and reduced appetite
- Jaw tension, teeth grinding (bruxism)
- Restlessness and muscle tension
- Insomnia and difficulty sleeping
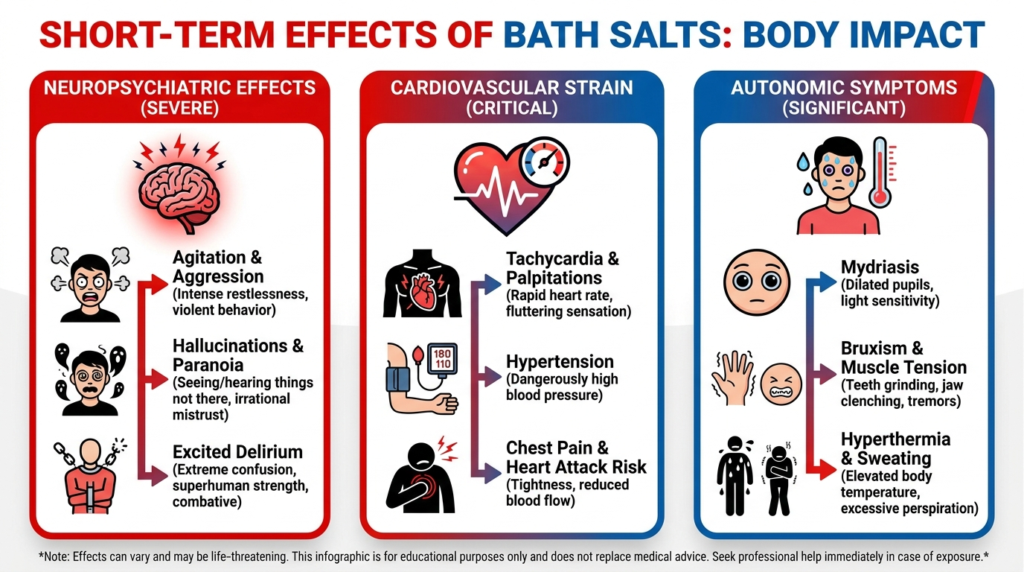
A Dutch poison center study of 3-MMC poisonings found that tachycardia occurred in 35% of cases, hypertension in 20%, and agitation in 19%, even in mono-intoxications where no other drugs were involved.
Side Effects and Acute Toxicity
The side effects of 2-MMC range from uncomfortable to life-threatening. Because direct human toxicity data for 2-MMC remain limited, the best evidence comes from closely related compounds like 3-MMC and mephedrone.
Common Adverse Effects
A comprehensive review of 3-MMC toxicity documented frequent adverse effects across cardiovascular, neurological, and psychiatric domains:
Cardiovascular symptoms:
- Palpitations and chest pain
- Rapid or irregular heartbeat
- Elevated blood pressure
- ECG abnormalities in some cases
Neurological symptoms:
- Headache and dizziness
- Uncoordinated movements or staggering
- Tingling sensations
- Reduced consciousness in severe cases
- Seizures or convulsions
Psychiatric symptoms:
- Anxiety, panic, and fear
- Agitation and aggression
- Confusion and disorientation
- Paranoid delusions
- Hallucinations (visual or auditory)
- Psychotic episodes
Other systemic effects:
- Profuse sweating
- Nausea and gastrointestinal distress
- Difficulty breathing
- Severe dehydration
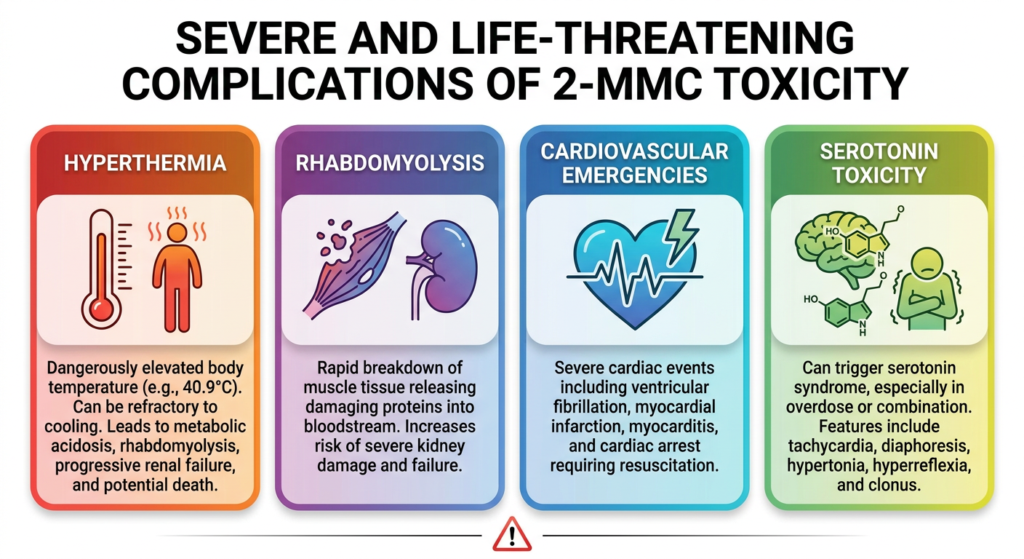
Severe and Life-Threatening Complications
When 2-MMC toxicity becomes severe, it can produce medical emergencies requiring intensive care. Evidence from synthetic cathinone poisonings shows several dangerous complications:
Hyperthermia: Dangerously elevated body temperature is one of the most serious complications. The 3-MMC review describes a fatal case with body temperature of 40.9°C lasting up to 20 hours, refractory to cooling measures, followed by metabolic acidosis, rhabdomyolysis, progressive renal failure, and death.
Rhabdomyolysis: This condition involves rapid breakdown of muscle tissue, releasing proteins into the bloodstream that can damage kidneys. A study comparing sympathomimetic toxicity found that 42% of patients developed rhabdomyolysis, and synthetic cathinone exposure specifically increased odds of severe rhabdomyolysis compared with other stimulants.
Cardiovascular emergencies: A Dutch cardiotoxicity case series documented severe cardiac events after synthetic cathinone use, including ventricular fibrillation requiring resuscitation, myocardial infarction, myocarditis, and cardiac arrest.
Serotonin toxicity: Although 2-MMC appears less serotonergic than mephedrone, it can still trigger serotonin syndrome, especially in overdose or when combined with other serotonergic drugs. A confirmed mephedrone serotonin syndrome case showed classic features including tachycardia, diaphoresis, hypertonia, hyperreflexia, clonus, and progression to hyperthermia.
| Complication | Key Features | Why It Matters |
|---|---|---|
| Hyperthermia | Body temperature above 40°C, refractory to cooling | Can trigger multiorgan failure, DIC, coma, death |
| Rhabdomyolysis | Muscle breakdown, dark urine, elevated creatine kinase | Leads to acute kidney injury, electrolyte disturbances |
| Cardiac events | Arrhythmias, chest pain, ECG changes, arrest | Can be fatal; requires immediate emergency care |
| Serotonin toxicity | Agitation, confusion, muscle rigidity, hyperthermia | Medical emergency requiring specific treatment |
2-MMC Overdose Risk
Direct 2-MMC overdose case data remain sparse, but the evidence from closely related cathinones provides clear warning signals. The 3-MMC toxicity review explicitly notes that because desired effects are short-lived, users often repeat administration within a single session, which may escalate overdose risk.
Why Overdose Risk is Higher Than It Appears
Several factors combine to make 2-MMC overdose more likely than users may realize:
Product misidentification: About half of supposed 3-MMC samples actually contained 2-MMC in early 2024 European drug-checking data. When users dose based on expectations for a different drug, they may take too much or redose too soon.
Extreme purity variation: A prospective drug-checking study found that powder purity ranged from 21% to 98%. Someone accustomed to weak product may accidentally consume several times more active drug when they encounter high-purity material.
Compulsive redosing: The short duration of 2-MMC creates strong pressure to redose. Each additional dose increases total drug exposure, cardiovascular strain, and risk of severe complications like hyperthermia and rhabdomyolysis.
Polydrug use: The 3-MMC review notes that many reported deaths and severe intoxications occurred after mixing 3-MMC with other psychoactive substances. Combining 2-MMC with alcohol, GHB, other stimulants, or serotonergic drugs multiplies risk.
Overdose Warning Signs
Someone who has taken 2-MMC or a product that may contain it needs urgent medical evaluation if they develop:
- Severe chest pain or pressure
- Very fast, irregular, or pounding heartbeat
- Extremely high body temperature with heavy sweating and agitation
- Severe confusion, disorientation, or inability to recognize surroundings
- Hallucinations, paranoia, or psychotic symptoms
- Seizures, convulsions, or uncontrollable muscle jerking
- Collapse, loss of consciousness, or inability to wake
- Severe muscle pain or dark-colored urine
- Difficulty breathing or bluish skin
These warning signs are consistent with severe synthetic cathinone toxicity documented in emergency medicine literature and require immediate professional care.
2-MMC Addiction and Dependence Risk
The 2025 systematic review concluded that 2-MMC and 3-MMC may have higher dependence risk than mephedrone because their shorter duration of action increases craving and frequent redosing. This is one of the strongest and most concrete conclusions available in the current evidence base.
Why Short Duration Increases Addiction Risk?
Drugs with rapid onset and short duration can be particularly habit-forming because they create a repeated cycle of reward, decline, and craving within a single use session. This pattern strengthens compulsive use through several mechanisms:
- Faster offset of desired effects creates stronger temptation to redose
- More frequent dosing produces more reinforcement cycles
- Greater relative dopaminergic activity (compared with serotonergic) fits stronger stimulant-seeking behavior
- Short action reduces the satiating or prosocial buffering effects seen with more balanced entactogens like MDMA
Real-World Evidence of Problematic Use
The Netherlands provides an important warning about how quickly methylmethcathinones can move from novelty to treatment burden.
Among nightlife youth aged 16 to 35, past-year 3-MMC use increased almost four-fold within two years, reaching 33.7% in 2022 and becoming the third most commonly used substance after cannabis and MDMA.
Even more striking, the number of people seeking treatment for problematic 3-MMC use in the Netherlands rose from 33 in 2021 to 330 in 2023. Since 2-MMC is now emerging as a replacement in the same market, similar patterns of escalating use and treatment demand are likely.
Vulnerable Populations
The systematic review notes that low price, high availability, and positive social media recommendations have attracted very young users aged 14 to 17, who are especially vulnerable to impulsive redosing and mental health complications.
Adolescents and young adults may be particularly susceptible to developing problematic use patterns because their reward systems are still developing and they have less experience recognizing warning signs.
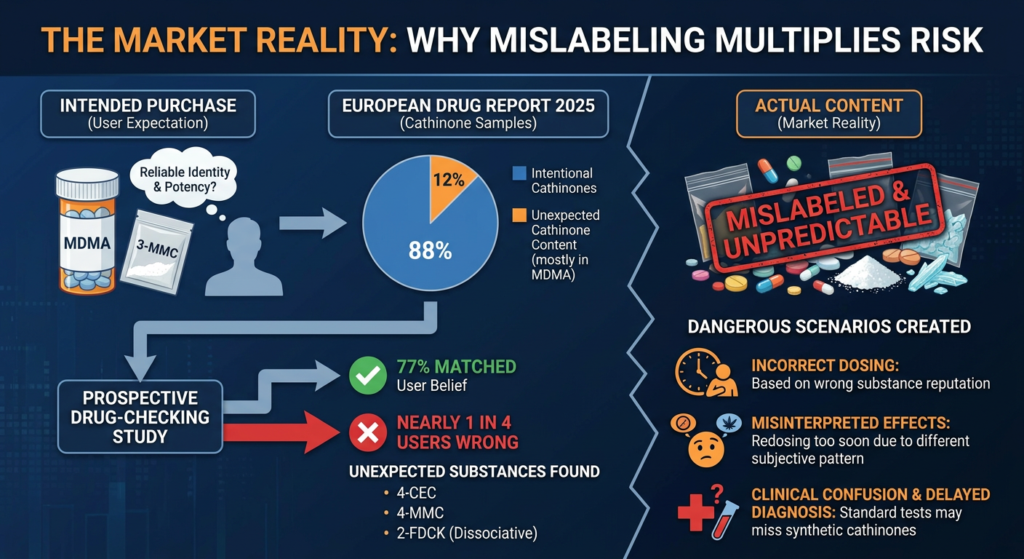
The Market Reality: Why Mislabeling Multiplies Risk?
One of the most important findings across the evidence is that 2-MMC risk is shaped not only by its pharmacology but by how it is sold. Drug toxicity becomes much harder to predict when users cannot reliably identify the compound or estimate potency.
The European Drug Report 2025 documented that among samples found to contain cathinones, 88% were intentionally submitted as cathinones, but the remaining 12% were mostly MDMA samples with unexpected cathinone content. This indicates both intentional use and adulteration into other stimulant markets.
A prospective drug-checking study found that only 77% of submitted samples matched what users believed they had purchased. Nearly one in four users were wrong about the identity of their product. Unexpected substances included 4-CEC, 4-MMC, and 2-FDCK, a dissociative drug pharmacologically very different from cathinones.
This widespread mislabeling creates several dangerous scenarios:
- Users may dose based on the reputation or expected duration of 3-MMC but receive 2-MMC instead
- Someone expecting MDMA may misinterpret the different subjective pattern of a cathinone and redose too soon
- Clinicians treating intoxication may not know which substance is actually responsible
- Standard drug tests may miss synthetic cathinones entirely, delaying proper diagnosis
Clinical Management of 2-MMC Toxicity
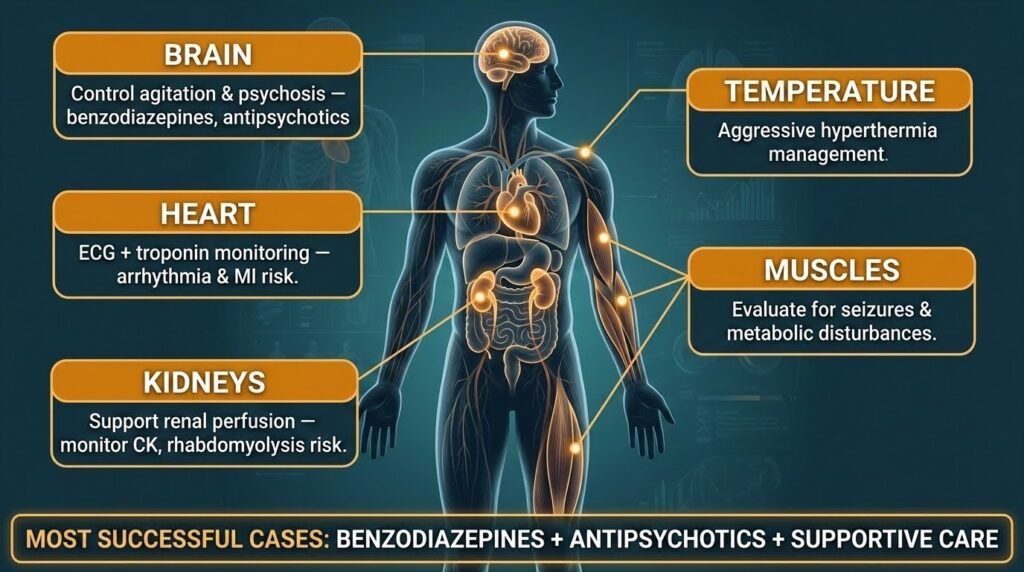
The best-supported emergency management priorities for severe stimulant and synthetic cathinone toxicity are aggressive IV fluids, rapid correction of hyperthermia, and benzodiazepines to reduce muscle activity and metabolic demand, according to rhabdomyolysis research.
Benzodiazepines are central to treatment because they reduce agitation, seizure risk, sympathetic overdrive, and excessive muscle activity that contributes to hyperthermia and rhabdomyolysis. Hyperthermia must be treated as time-critical because delayed control can lead to renal failure, disseminated intravascular coagulation, coma, and death.
In suspected severe 2-MMC intoxication, clinicians should monitor temperature, heart rate and blood pressure, ECG changes, creatine kinase, renal function, electrolytes, acid-base status, and mental status. The 3-MMC review notes that LC-MS/MS is a standard method for identifying the specific drug responsible for intoxication, which matters because routine screens may miss novel cathinones.
Why 2-MMC is a Growing Public Health Concern?
The European Union Drugs Agency reported unprecedented imports and seizures of synthetic cathinones, with annual quantities increasing to 37 tonnes in 2023, with preliminary data suggesting continued large quantities through 2024. In 2024 and 2025 EU communications, synthetic cathinones are explicitly described as gaining ground on Europe’s stimulant market.
By 2026, EU legal measures had brought 2-MMC under control across the EU, indicating that policymakers judged the substance to present sufficient harm or public health risk to warrant formal action. That legal status reinforces that 2-MMC is no longer viewed as a marginal or purely hypothetical issue.
A recurring pattern in new psychoactive substances is that market penetration often precedes clear treatment pathways and public recognition. By the time clinicians and users understand a new cathinone well, the market may already have shifted again. This is why substitution data and analog toxicology are so important for understanding emerging risks.
What You Need to Know About 2-MMC?
The available evidence supports several clear conclusions about 2-MMC:
It is a real and growing presence in the European stimulant market, not an isolated niche drug. It is frequently encountered through substitution, especially in products sold as 3-MMC.
It has a pharmacological profile similar to mephedrone with comparable dopaminergic but less serotonergic activity, and shorter duration than 4-MMC. This combination likely increases craving and redosing, raising dependence risk.
Closely related methylmethcathinones can produce severe toxicity including severe hypertension, psychosis, seizures, hyperthermia, rhabdomyolysis, cardiac arrest, and death. While direct 2-MMC case data remain limited, the analog evidence is strong enough to justify serious concern.
Street supply is highly unreliable with major purity variation and frequent mislabeling. About half of products sold as 3-MMC in early 2024 actually contained 2-MMC, and purity ranged from 21% to 98%.
The most defensible overall judgment is that the major risk of 2-MMC lies in its combination of stimulant reinforcement, short action, high redosing pressure, and supply-chain unreliability. That combination is exactly what produces both addiction escalation and acute toxicity in the real world.
If you or someone you know is struggling with stimulant use or experiencing concerning symptoms after taking 2-MMC or related substances, our professional help is available. Thoroughbred Wellness & Recovery offers comprehensive addiction treatment including medical detox, dual diagnosis care, and evidence-based therapies designed to support lasting recovery.