Why Lawyer Burnout Alcohol Use is Increasing? Affects & Risk
Georgia attorneys are facing a hidden crisis. The 2016 ABA–Hazelden study found that 20.6% of lawyers screened positive for hazardous or potentially alcohol-dependent drinking, while depression, anxiety, and stress affected substantial portions of the profession.
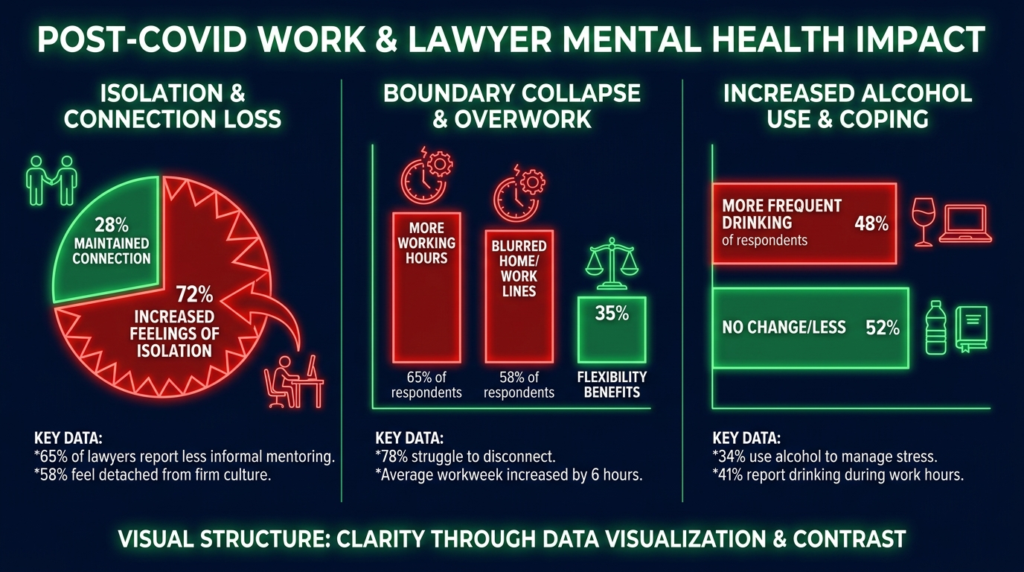
Post-COVID conditions have intensified these risks by eroding work boundaries, increasing isolation, and making impairment harder to detect in hybrid practice settings.
This article explains how burnout drives alcohol misuse among Georgia lawyers and what warning signs matter most.
The National Baseline: Lawyer Alcohol Use Was Already High Before COVID
The legal profession entered the pandemic with a well-documented substance use problem. The 2016 landmark study surveyed 12,825 licensed, employed attorneys and revealed troubling patterns. Beyond the 20.6% hazardous drinking rate, the research documented significant mental health concerns including depression, anxiety, and chronic stress.
What made this study particularly important was its scope and methodology. The ABA describes it as landmark research because it simultaneously measured both substance use and behavioral health concerns nationally for the first time. Before 2016, the profession relied largely on anecdote and regional data. This study provided empirical proof that lawyer distress was structural, not isolated.
Younger lawyers showed especially high risk. The findings reversed earlier assumptions by showing that attorneys newer to practice had the highest alcohol abuse rates, not senior practitioners. This pattern matters for Georgia because many younger attorneys were socialized into the profession during or after the shift to remote work, potentially missing crucial in-person mentoring and peer observation.
How COVID Changed the Risk Environment for Georgia Lawyers?
The pandemic did not create lawyer burnout and alcohol misuse. It transformed the conditions under which these problems develop and persist. Georgia’s legal system adapted quickly to remote operations. The Judicial Council of Georgia conducted its August 14, 2020 general session by remote conferencing, illustrating how deeply governance and operational routines changed during the pandemic period.
These shifts had unintended consequences. Hybrid and remote work arrangements made mental health and substance use problems much more difficult to detect because lawyers are no longer observed regularly. Problems are more likely to grow when someone is isolated or only around colleagues a couple of days per week, since loneliness and isolation are well-known risk factors for addiction.
The profession recognized these changes were significant enough to require new research. In June 2025, the ABA and Krill Strategies launched a new national lawyer mental health project specifically to provide a 10-year update to the 2016 study. The ABA stated this was critically needed because of substantial shifts in the legal profession over the past decade, including significant changes resulting from the COVID-19 pandemic.
The Boundary Collapse Problem
One of the clearest post-COVID patterns is the disappearance of natural stress buffers. Commutes, lunch breaks, and office transitions once created psychological separation between work and home. Remote work eliminated these pauses. When a lawyer finishes a difficult call and immediately starts dinner prep in the same room, there is no decompression space.
This boundary collapse shows up in recent workplace surveys. A 2025 survey found that 65.5% of lawyers and staff said billable-hour pressures were negatively affecting mental wellbeing, while 56.3% said always being on call harmed wellbeing. About 73% reported their work environment contributed to mental health issues over time.
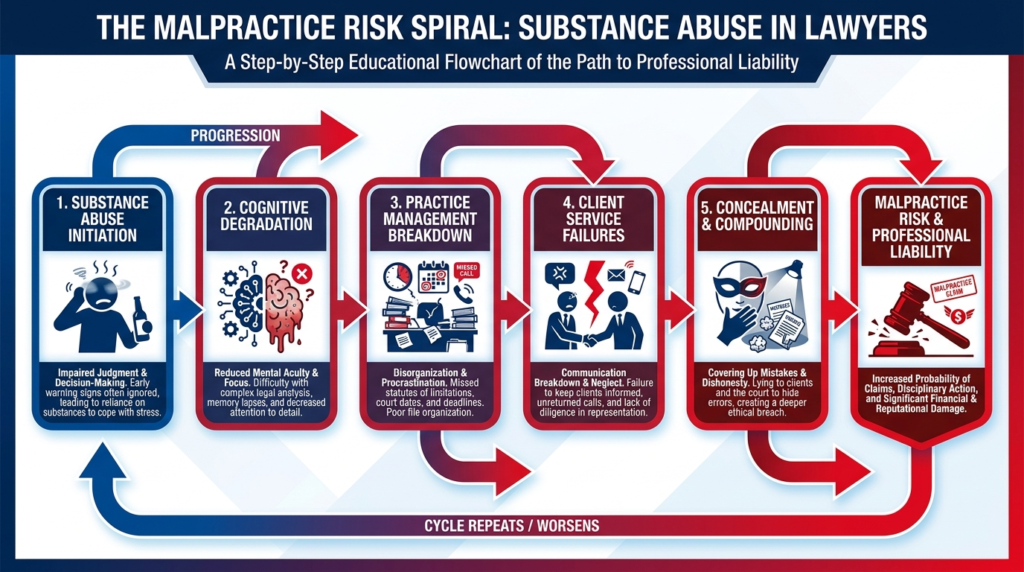
The Burnout to Alcohol Pathway: How Chronic Stress Becomes Substance Risk?
Burnout is not simply feeling tired or stressed. It is a state of emotional exhaustion, cynicism, and reduced professional effectiveness that develops when work demands consistently exceed recovery capacity. For Georgia attorneys, burnout functions as a major transmission mechanism linking work conditions to alcohol misuse.
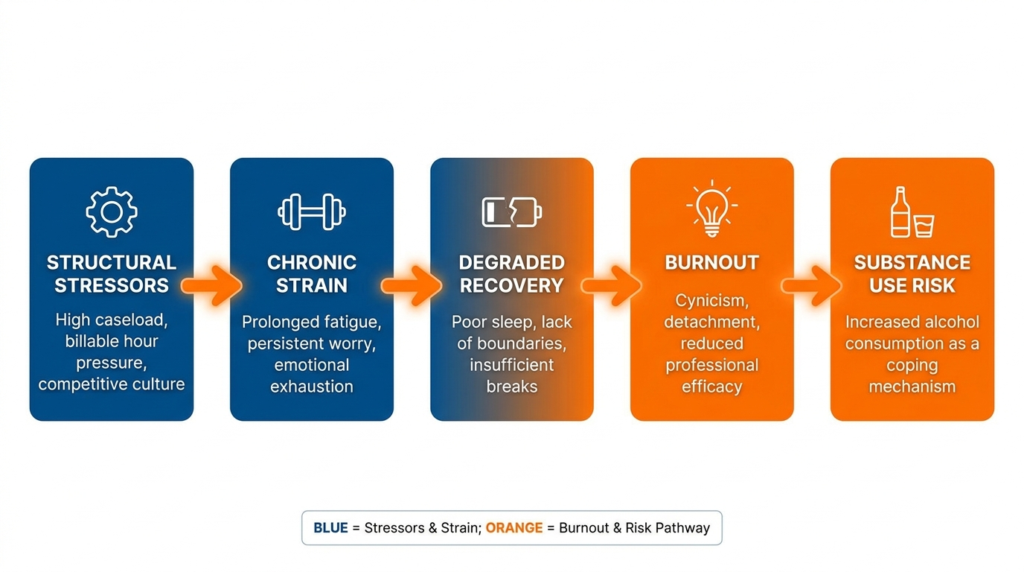
The pathway works through several connected steps:
Structural stressors increase chronic strain: Billable expectations, constant availability, blurred boundaries, overcommitment, and work-family conflict create sustained pressure. Georgia lawyers face the same economics-driven dynamics seen nationally: firms need billable hours, clients expect immediate responsiveness, and technology makes round-the-clock availability technically possible.
Chronic strain degrades recovery: When lawyers have less true time off, more rumination, less detachment, and sustained physiological arousal, the body and mind cannot fully reset. Sleep quality declines. Irritability increases. Cognitive resources deplete.
Degraded recovery contributes to burnout: Exhaustion becomes chronic. Lawyers develop cynicism or emotional detachment as a protective response. Work that once felt meaningful starts feeling mechanical or overwhelming.
Burnout elevates substance use risk: At this stage, alcohol can seem like a practical solution. It is fast, socially acceptable in legal culture, and privately accessible. Lawyers may use alcohol as self-medication, numbing, or a way to force mental shutdown after a day of sustained activation.
This is not speculation. Research shows that workplace attitudes and permissiveness toward alcohol significantly influence the likelihood of problematic drinking among lawyers. When professional culture normalizes alcohol-centered networking and stress relief, it reinforces both access and legitimacy.
Warning Signs Georgia Lawyers and Employers Should Watch For!
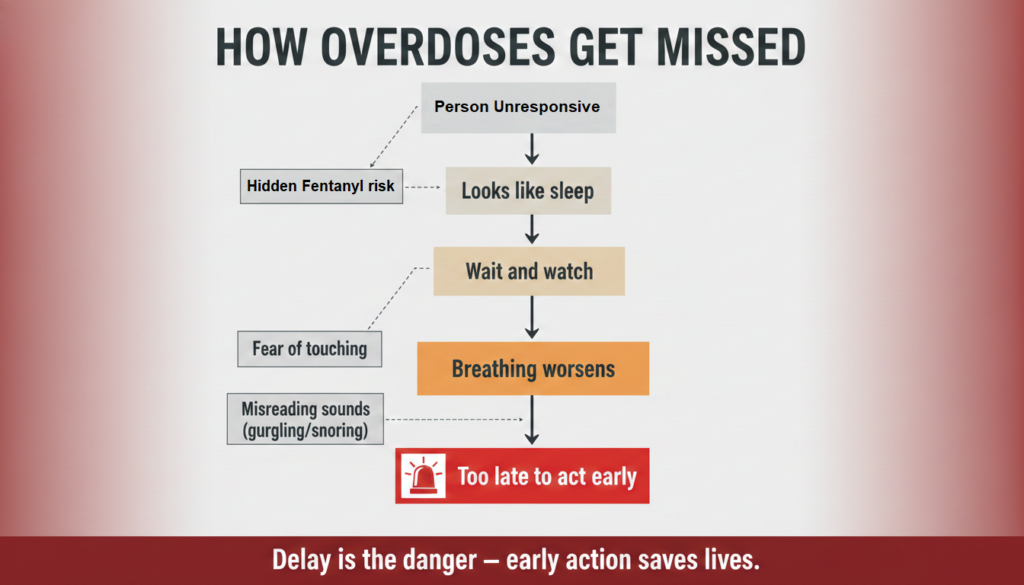
Post-COVID impairment often develops gradually rather than dramatically. The most important warning signs are not sudden crises but slow behavioral shifts that accumulate over time.
Early behavioral indicators
- Consistently working through lunch, nights, or weekends without restorative boundaries
- Regular comments about needing alcohol to unwind or decompress
- Increased isolation from colleagues, especially in hybrid settings
- Camera-off patterns or withdrawal from optional team contact
- More defensiveness when asked about workload or stress
- Declining reliability in email response, filings, or follow-up
Performance warning signs
- Decline in work quality or attention to detail
- Missed deadlines or near misses that were previously rare
- More client complaints or dissatisfaction
- Slower turnaround on routine tasks
- Uncharacteristic mistakes in detail-heavy work
- Overpromising and underdelivering
Emotional and alcohol-related indicators
- Greater irritability, cynicism, or emotional detachment
- Heightened anxiety, hopelessness, or shame
- Loss of motivation or flattening of affect
- Progressive increase in nightly drinking
- Drinking earlier in the day or more frequently to take the edge off
- Concealment, minimization, or joking defensiveness about drinking
One particularly revealing pattern appears in remote work settings. A lawyer may lose the commute and lunch break that once functioned as natural stress buffers. As those pauses disappear, stress escalates. Evening drinking increases from one glass of wine to a bottle.
Work quality declines. Clients begin complaining. By the time the problem becomes visible, functioning has already eroded significantly.
What Georgia’s Lawyer Assistance Infrastructure Reveals About the Problem?
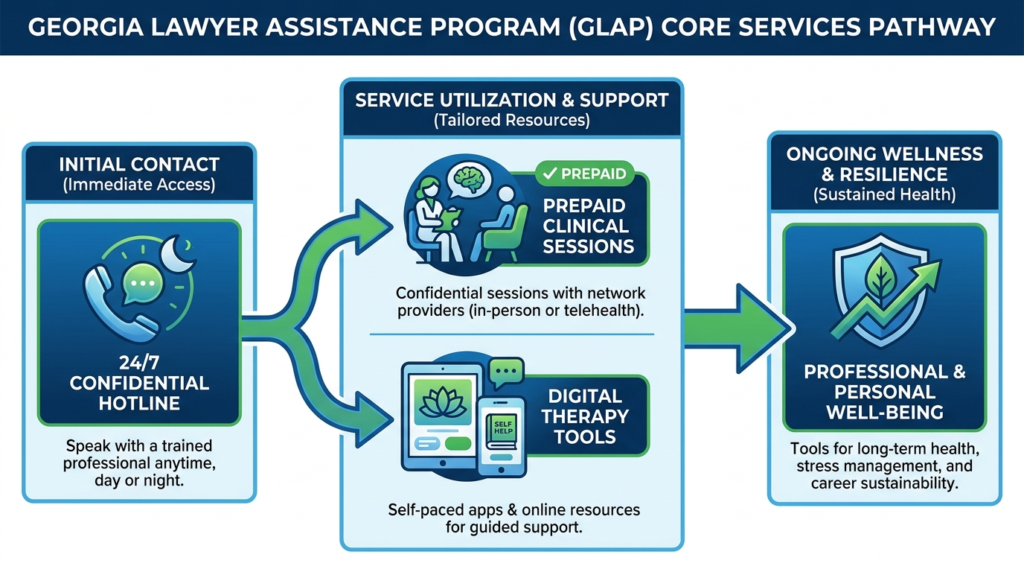
Georgia has built a comparatively mature support system for lawyer wellbeing. The State Bar of Georgia maintains a Center for Lawyer Wellbeing, a confidential Lawyer Assistance Program, a 24/7 hotline, six prepaid clinical sessions per year, digital access tools, text therapy, digital cognitive behavioral therapy, virtual group support, and Georgia Lawyers Helping Lawyers, a confidential peer-support program.
This infrastructure is meaningful. It shows that Georgia’s governing professional body recognizes lawyer distress as widespread and persistent rather than episodic. The Bar explicitly identifies depression, stress, alcohol or drug abuse, family problems, and psychological issues as concerns affecting lawyers and directs members to immediate confidential help.
The scope of services suggests broad expected demand. A system built only for rare emergencies would not typically include multiple digital modalities, virtual groups, text therapy, and prepaid counseling sessions. The structure also reflects post-COVID adaptation. Remote and digital access options are particularly relevant for lawyers working hybrid schedules, living outside metro centers, or reluctant to seek visible in-person help.
The Center for Lawyer Wellbeing prominently markets the “#UseYour6” message referencing the six prepaid counseling sessions available to members. The need to campaign for use of available sessions strongly implies an operational concern not just with the existence of services, but with underutilization, likely due to stigma, denial, or uncertainty.
Why High-Functioning Lawyers Delay Seeking Help?
Legal culture still discourages visible need. Lawyers are trained to project competence, manage adversarial conflict, and solve problems independently. This professional identity can become a barrier to help-seeking.
The 2016 study found that lawyers often do not seek help because they fear someone will find out, discredit them, or affect their license. Some law students considering treatment feared exclusion from faculty, peers, administrators, and bar associations due to mental health history.
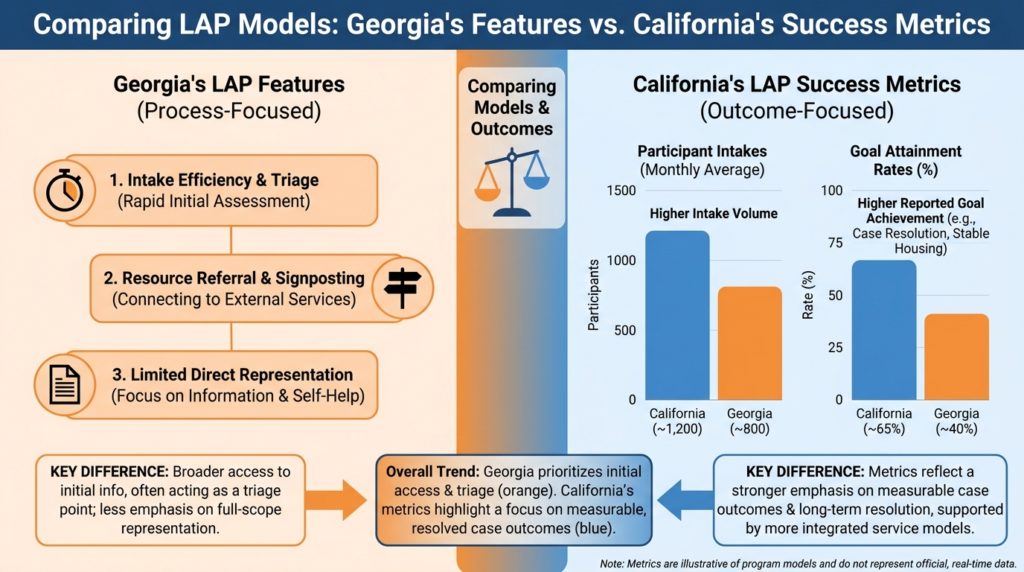
These fears have large practical consequences. They mean lawyers may delay help until distress becomes severe, by which point maladaptive coping patterns may already be entrenched. The State Bar of California offered all lawyers at least two free counseling sessions, yet only about 200 of more than 183,000 active members used the benefit at a given time.
This is powerful evidence that availability alone is not enough. A resource can exist and still go largely unused if the profession teaches lawyers that using it is risky, shameful, or career-damaging.
The Concrete Risk Profile for Georgia Attorneys Post-COVID
Based on the strongest available evidence, the most defensible conclusion is this: post-COVID impairment risk among Georgia lawyers is probably being underdetected rather than overstated. The biggest practical threat is not dramatic collapse but slow, high-functioning deterioration driven by burnout, isolation, and stress-linked alcohol use.
This opinion is supported by five converging facts:
The national baseline already showed serious lawyer alcohol risk: If 20.6% of attorneys nationally screened positive for hazardous or problematic drinking in the landmark baseline study, the profession started from a high-risk position even before COVID’s structural disruptions.
Post-COVID work arrangements make those problems harder to observe: Hybrid and remote practice make mental health and substance use problems more difficult to detect while increasing loneliness and isolation, both known risk factors.
The profession itself believes the old data are outdated: The ABA launched a 2025 update because of major profession-wide changes, including post-COVID shifts and technology pressure.
Georgia has built significant support infrastructure: Georgia’s Center for Lawyer Wellbeing, peer support, and LAP with multiple digital modalities imply that need is large enough and persistent enough to warrant institutional investment.
The profession still tends to respond too late: The warning patterns highlighted by research often culminate in declining work quality and client complaints, meaning detection commonly happens after functioning has already eroded.
What Georgia Lawyers Can Do Now?
If you are a Georgia attorney experiencing chronic stress, boundary erosion, or increasing reliance on alcohol to decompress, you are not alone.
The State Bar of Georgia’s Lawyer Assistance Program is confidential and already paid for in part through member benefits. It explicitly covers stress, anxiety, depression, workplace conflict, family problems, and other issues, not just addiction crises.
High-priority self-monitoring questions include:
- Have I stopped taking restorative breaks that used to structure my day?
- Am I drinking to regulate emotion, sleep, or decompression?
- Have I become more isolated since moving to hybrid or remote work?
- Am I more irritable, numb, cynical, or detached from clients?
- Has my work become slower, sloppier, or more effortful?
- Have I delayed seeking help because I think I am still functioning?
The most important insight from the research is that waiting until you are visibly impaired is waiting too long. Early intervention works better, feels less overwhelming, and protects both your wellbeing and your practice.
If you or a colleague is struggling with burnout, stress, or alcohol use, confidential support is available. Georgia’s Lawyer Assistance Program offers immediate help at 800-327-9631, and you can also access Thoroughbred’s dual diagnosis treatment that addresses both substance use and mental health concerns together.